The concept of “deformity” in orthopedics is a very general concept and can occur in all structures that make up the musculoskeletal system. In many diseases affecting the musculoskeletal system, we may encounter deformities in the lower and upper extremities. These include congenital bone anomalies; disorders caused by trauma; various metabolic diseases and genetically based skeletal dysplasias are the most common. In addition, there are deformities that occur during child development and are accepted as normal variations of physiological growth, but are seen as a reason for applying to outpatient clinics with panic and fear by families. In general, lower extremity deformities take up more space, especially in pediatric orthopedic practice, as they are more common and affect the daily functions of the person more.
It is important to distinguish whether deformities seen in the pediatric age are a condition that needs to be treated or are part of normal development. Making this decision not only protects the child from unnecessary examinations and treatments, but also eliminates the unnecessary haste and fear that the family will experience. Mastering the details of the child’s musculoskeletal development and a careful examination are sufficient to make this distinction.
There are different techniques that can be applied after a problem that needs to be treated with a surgical method is revealed. While some of these techniques are specific to childhood, most of them can be applied to deformities seen in adult patients.
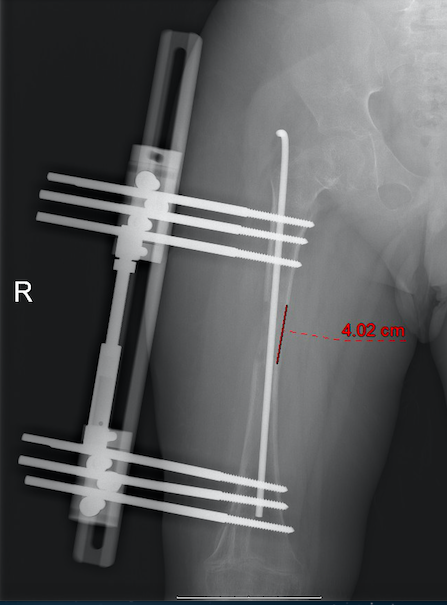
External Fixators
External fixators are systems that hold the bone with externally placed nails and wires. After the bone is broken/cut from the appropriate area, correction is provided by moving the bone pieces by means of nails. Different external fixators have been developed according to the type and region of the deformity and have been put into daily use. It is possible to lengthen the bone and angle it in different directions with external fixators placed in accordance with the specific rules for the desired correction. Computer-assisted external fixators, which have become popular in recent years, allow all these corrections to be planned precisely and applied on the patient.
The most disturbing feature of external fixators for patients is the fixation materials that move from the skin to the bone. These areas, which have the potential to cause skin problems, pain and soft tissue infections at varying rates depending on the area of application, should be dressed regularly. Due to this feature, it may cause disruption of the physical therapy program from time to time.
Despite these disadvantages, it is possible to achieve very successful results in areas where other methods cannot be applied and especially in patients who need bone lengthening with correction.
Clamp system (growth routing)
The method known as growth-directing therapy is a surgical method specific to childhood. Correction is achieved by controlling the growth areas of the child’s bone and suppressing the growth in an asymmetrical manner. The patient must have sufficient growth potential in order for this technique, which works with the mechanism of suppression of cellular activity in the growth plates, to be successful. Therefore, the technique is more likely to fail in girls over 12 years old and boys over 14 years old. Before applying this technique, it should be ensured that the growth plate is healthy.
The most important advantage of the technique is that it can be corrected without the need to break/cut the bone. After the surgery, patients can walk on the first day and can quickly return to their daily life activities. The surgical incision applied is quite small. Surgery pain can be easily controlled. The most important issue for families to keep in mind is that the planned recovery will occur in parallel with the growth of the child after the surgery.
Plates and screws placed for growth-directing therapy are removed with a second surgery when recovery is complete. Therefore, the improvement in the patient should be followed regularly (every 4-6 months).
Use of plates and screws
Corrections using plates and screws are procedures in which the bone is cut/broken and necessary corrections are made during the surgery, unlike growth-directing treatments. These are the methods that can be applied in most of the bone deformities. After the bone is cut, the correction required by the patient is made and the bone is fixed in that position by means of plates and screws. In order to make a solid fixation in the bone, an average of 6-8 perforated plates are used and longer skin incisions are needed for their placement.
Although the bone is fixed with plates and screws, this fixation does not allow the patient to immediately put a load on the involved extremity. For this reason, patients move with a support such as a walker or crutches without pressing the relevant side for 4-6 weeks. The healing of the bone incision should be followed regularly. Walking activity is regulated by giving a load parallel to the healing of the bone.
Use of intrabony nails
The long bones in the human body are roughly cylindrical, with holes in the middle to accommodate nails. The length and thickness of the nail that can be applied may vary from person to person. As in the plate/screw correction technique, the bone is cut from the appropriate area(s) in the bone-in-nail correction technique, ensuring adequate correction and bone fixation is done with nails.
Activation of bone growth plates in childhood limits the use of standard intraosseous nails. The main reason for this is the potential of the nails to damage the bone growth areas and negatively inhibit the growth of the bone. For this reason, nails are more suitable options for young adults and adult patients with closed growth plates.
The use of small skin incisions during application results in more cosmetically acceptable scar tissue. Patient mobilization can be done quickly.